
Can Low Iron Cause ADHD Symptoms in Children?
✨ At a Glance
Low ferritin (stored iron) can reduce dopamine production, causing symptoms that closely resemble ADHD, including inattention, impulsivity, and restlessness
Iron is also required for serotonin and melatonin, meaning low stores can contribute to anxiety, mood swings, and poor sleep
A child can have low ferritin while haemoglobin remains completely normal, and be told their iron is "fine"
Australian pathology defines iron deficiency in children as ferritin below 20 µg/L, but functional practitioners often aim closer to 50 µg/L to support brain function
Ferritin is not included in a standard blood count. It must be specifically requested
Identifying and addressing low ferritin can meaningfully shift behaviour, mood, and sleep in some children
Low iron can produce symptoms that closely resemble ADHD in children, including inattention, impulsivity, restlessness and poor sleep. This happens because dopamine, the neurotransmitter most closely linked to attention and impulse control, depends on an iron-requiring enzyme to be made. A child's ferritin (stored iron) can be low enough to affect brain function while their haemoglobin remains completely normal, which is why many children are told their iron is "fine". Research has consistently found lower ferritin in children diagnosed with ADHD, and iron supplementation may reduce symptom severity in some children, even without anaemia.
If your child has been diagnosed with ADHD, or you suspect they might have it, you have probably spent a lot of time trying to understand what is driving their symptoms. The restlessness. The emotional volatility. The difficulty settling at night. The meltdowns that seem to come out of nowhere.
What many parents are not told (and what standard paediatric testing often misses) is that low iron stores can produce symptoms virtually indistinguishable from ADHD.
Not low enough to cause anaemia. Not low enough to flag on a standard blood count. But low enough to quietly undermine the very brain chemistry that governs your child's attention, mood, and sleep.
This article walks through the science of why this happens, what to look for, and why the conventional "normal range" may not be telling the full story.
What is ferritin, and why does it matter for your child's brain?
Ferritin is the protein your body uses to store iron. When we test ferritin levels in blood, we are getting a snapshot of how much iron is sitting in reserve available to be drawn on when the body needs it.
Most GPs test for iron deficiency by checking haemoglobin, the protein in red blood cells that carries oxygen. Haemoglobin only drops once iron stores are significantly depleted. By the time haemoglobin is low, ferritin has often been running low for months.
This gap matters enormously in children, because the brain does not wait for anaemia before being affected.
Iron is required to produce several key neurotransmitters, the chemical messengers that govern how your child thinks, feels, behaves, and sleeps. When ferritin is low, even if haemoglobin is perfectly normal, those neurotransmitter pathways can become compromised.
This is why a child can be told their iron is "fine" while continuing to struggle.
The dopamine connection: why low iron looks like ADHD
Dopamine is the neurotransmitter most closely associated with ADHD.
It plays a central role in:
Sustaining attention on tasks that are not immediately rewarding
Regulating impulse control
Supporting motivation and follow-through
Moderating hyperactivity and restlessness
The production of dopamine depends on an enzyme called tyrosine hydroxylase. This enzyme is iron-dependent, meaning it requires adequate iron to function properly.
When ferritin levels are low, tyrosine hydroxylase activity can be reduced, which means dopamine synthesis may be impaired.
The result? A child who cannot focus, struggles to sit still, acts before thinking, and finds it nearly impossible to complete tasks they find unrewarding. A child who looks, in every practical sense, like they have ADHD.
Research has consistently found lower ferritin levels in children diagnosed with ADHD compared to neurotypical children, with some studies showing that iron supplementation can meaningfully reduce ADHD symptom severity, even in children without clinical anaemia.
This does not mean every child with ADHD has low iron. But it does mean that iron status is worth investigating before assuming symptoms are purely neurodevelopmental in origin.
"I see children whose ferritin sits at 22 µg/L being told their iron is fine, when their dopamine pathway is quietly running on empty. The conventional cut-off was designed to catch anaemia. It was never designed to answer the question parents are actually asking: does my child have enough stored iron to think, regulate, and sleep?"
— Ayelet Center, Naturopath, Botanic Artisan
Serotonin, mood, and emotional regulation
Serotonin is less often discussed in the context of ADHD, but it plays a significant supporting role in your child's emotional life.
It influences:
Emotional resilience and the ability to tolerate frustration
Baseline mood and calmness
Anxiety levels
The capacity to recover from upsets
Like dopamine, serotonin is produced via an iron-dependent enzyme, tryptophan hydroxylase. When iron stores are low, serotonin production may be reduced.
In practice, this can look like a child who is more irritable than expected, quicker to become overwhelmed, prone to anxiety, or emotionally reactive in ways that feel disproportionate to the situation.
It can also look like a child who is sad or flat without obvious cause. Or one who melts down over small transitions and cannot easily be consoled.
These mood and regulation difficulties are often attributed to "big emotions", temperament, or anxiety disorders. Iron is rarely on the list of things to investigate.
Sleep disturbances: the melatonin link
Here is where the picture becomes even more layered.
Serotonin is the precursor to melatonin, the hormone responsible for initiating and maintaining sleep. This means that when serotonin is compromised by low iron, melatonin production can also be affected.
Many children with low ferritin are described by their parents as "tired but wired". They are clearly exhausted, but they cannot switch off. They take a long time to fall asleep, wake repeatedly through the night, or wake early feeling unrested.
There is also a well-established connection between low iron and restless legs syndrome in children, an uncomfortable, crawling sensation in the limbs that is worse at rest and relieved by movement. Children often cannot articulate this clearly. They say their legs feel "funny" or "itchy inside". They kick their covers, climb in and out of bed, and struggle to settle.
Poor sleep then compounds every other symptom. A child who is not sleeping well will have even less capacity to regulate attention, behaviour, and emotions during the day. The cycle is self-reinforcing.
Signs your child may have low ferritin
Low ferritin does not always look the way people expect. Because haemoglobin can remain normal, parents are often told the iron is fine and sent home.
Signs worth taking seriously include:
Difficulty sustaining attention, particularly on non-preferred tasks
Impulsivity and hyperactivity
Irritability, emotional volatility, or frequent meltdowns
Anxiety or social withdrawal
Fatigue that is inconsistent with sleep quantity
Difficulty falling asleep or restless, unsettled nights
Restless legs or complaints of discomfort in the limbs at night
Pale skin or persistent dark circles under the eyes
Picky eating, particularly low intake of red meat
Frequent illness suggesting immune vulnerability
No single sign is diagnostic on its own. But when several of these are present together, particularly alongside behavioural or attentional difficulties, it is worth investigating iron status more thoroughly. A simple ferritin test is a good place to start — you can find out more about functional testing and what we look at in clinic. If several of these signs sound familiar, a free 10-minute clarity call is an easy first step. Book here.
Why ferritin is so often missed
There are a few reasons low ferritin frequently goes undetected in children.
First, ferritin is not included in a standard full blood count. It must be specifically requested. Many routine paediatric blood panels do not include it.
Second, even when ferritin is tested, results are often interpreted using broad population-based reference ranges. These ranges are designed to identify disease, not optimal function. A child can fall within the "normal" range and still not have enough stored iron to support healthy neurotransmitter production.
Third, symptoms are frequently attributed to behaviour, temperament, or neurodevelopmental conditions without investigating whether an underlying physiological driver might be contributing.
The result is that many children with meaningful functional iron deficiency never have it identified or addressed.
What ferritin level should we be aiming for?
This is where integrative and naturopathic practitioners often differ from conventional medicine.
In Australia, iron deficiency in children is conventionally defined as ferritin below 20 µg/L (equivalent to ng/mL), based on guidelines from bodies including Australian Red Cross Lifeblood. Most standard pathology reports will not flag a result as low until it falls beneath this threshold, and many laboratories use an even lower cut-off.
Australian research from SA Pathology, drawing on over 54,000 paediatric iron studies at the Women's and Children's Hospital, proposed that the functional lower reference limit should be at least 26 µg/L for children under 13, and at least 39 µg/L for adolescents aged 13 to 19. In other words, the researchers found that the conventional cut-off does not reflect the level at which iron deficiency begins to affect red cell measures.
In clinical practice, when looking at brain function, behaviour, and mood in children, many integrative and naturopathic practitioners aim for ferritin levels closer to 50 µg/L as a functional target.
This is not a hard rule, and every child needs to be assessed individually. But the question being asked is different: not "is this child anaemic?" but "does this child have enough stored iron to support optimal brain development and neurotransmitter production?"
Those are two very different questions, and they often have different answers.
Why does low iron develop in children?
Low ferritin rarely appears without reason. Understanding why it has developed is essential to addressing it properly.
Common contributing factors include:
Dietary: Low intake of haem iron (found in red meat and organ meats), high dairy intake (calcium competes with iron absorption), insufficient vitamin C to support absorption, or picky eating patterns that significantly limit food variety.
Digestive:Low stomach acid reduces the conversion of iron into its absorbable form. Gut inflammation, increased intestinal permeability, or microbiome imbalance can all impair iron absorption even when dietary intake appears adequate. This same gut inflammation is also a common driver of conditions like eczema in children. The digestive and immune systems are rarely separate issues.
Demand: Periods of rapid growth significantly increase the body's iron requirements. Children who grow quickly may deplete stores faster than they replenish them.
Chronic inflammation or infection: Ongoing immune activation — including in conditions like PANS/PANDAS, can drive iron into storage as a protective mechanism, reducing its availability to the brain and other tissues.
Addressing the underlying cause is just as important as restoring the deficiency itself. Without it, iron levels may improve temporarily and then decline again.
A note on supplementation
Iron supplementation should always be guided by testing and overseen by a qualified practitioner.
Iron is not a benign supplement to take liberally. Too much iron can be harmful, and the form, dose, and timing of supplementation matters considerably for both efficacy and tolerability. Some children absorb iron well from food with targeted dietary changes alone. Others need supplemental support, and the right product and protocol depends on the individual.
It is also worth investigating the underlying cause before supplementing. If absorption is impaired, supplementing without addressing the digestive picture will often yield limited results.
The bigger picture
Low ferritin is often one piece of a more complex picture.
In clinical practice, children presenting with ADHD-like symptoms, emotional dysregulation, anxiety, or sleep difficulties rarely have a single root cause. Iron may be a significant contributor, sometimes the primary one, but it typically sits alongside other factors: gut health, nervous system regulation, inflammatory burden, other nutrient deficiencies, and environmental and lifestyle considerations.
The value of investigating iron specifically is that it is accessible, testable, and, when low genuinely addressable. Many families find that restoring iron levels is a meaningful turning point: the moment things begin to shift in ways they had not expected.
More settled sleep. Softer moods. A child who is more available, more regulated, more themselves.
That does not require waiting years for a diagnosis or committing to a medication trial. It requires good testing, a practitioner willing to look beyond conventional reference ranges, and a care plan that treats your child as an individual.
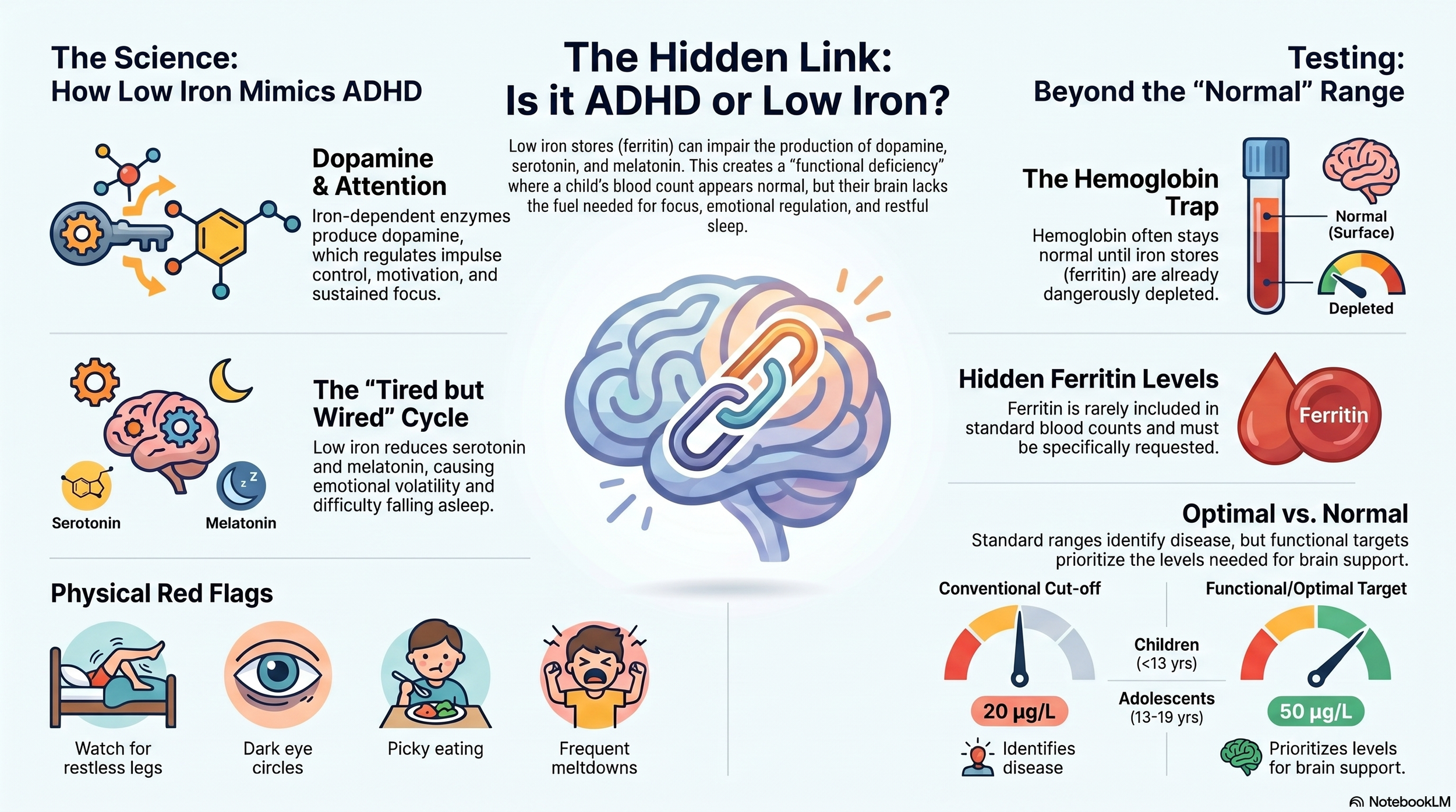
Illustration showing how low iron stores affect attention, mood and sleep in children
Frequently asked questions
Can low iron cause ADHD in children? Low iron does not cause ADHD as a neurodevelopmental condition, but it can produce symptoms that closely resemble ADHD, including inattention, impulsivity, and hyperactivity, by reducing dopamine production. In children with diagnosed ADHD, low ferritin may be amplifying symptoms.
What ferritin level is considered optimal for children's brain health? Australian pathology guidelines define iron deficiency in children as ferritin below 20 µg/L, but Australian research suggests the functional threshold — the point at which iron deficiency begins to affect haematological markers — may be closer to 26 µg/L for children under 13 and 39 µg/L for adolescents. Many integrative practitioners use a functional target closer to 50 µg/L when assessing brain health, mood, and behaviour.
Can low ferritin cause anxiety in children? Yes. Iron is required for serotonin production, which plays a key role in emotional regulation and anxiety. Low ferritin may contribute to heightened anxiety, irritability, and difficulty managing stress.
How does low iron affect sleep in children? Low iron can reduce both serotonin and melatonin production, making it difficult for children to fall or stay asleep. It is also strongly associated with restless legs syndrome, which frequently disrupts sleep in children.
Does my child need to be anaemic to have low ferritin? No. Ferritin can be low while haemoglobin remains normal. This is sometimes called functional iron deficiency. Because ferritin is not routinely tested, it is frequently missed.
Brugnara, C., Oski, F.A., and Nathan, D.G. (2018). Ferritin as a functional biomarker of iron status in children and young adults. British Journal of Haematology. SA Pathology, Adelaide Women's and Children's Hospital.
URL:https://onlinelibrary.wiley.com/doi/10.1111/bjh.15127
Does This Sound Like Your Child? If your child is struggling with what you've just read about, you're not alone. Early, gentle support can make a meaningful difference. Book a Free Clarity Call - no obligation, just clarity and next steps.
About the author
Ayelet is a naturopath, herbalist, homeopath, and nutritionist with a specialist focus on paediatric complex conditions, including PANS/PANDAS, gut health, immune dysfunction, and nervous system dysregulation. She practices at Botanic Artisan Bespoke Holistic Health, Sydney, and offers telehealth consultations across Australia. Ayelet works with children whose symptoms have often gone unexplained or unresolved through conventional pathways, and takes a thorough, whole-child approach to identifying and addressing the underlying drivers of behaviour, mood, attention, and sleep.
If you are concerned about your child's iron levels or would like to explore whether low ferritin may be contributing to their symptoms, an initial consultation can help you understand the full picture. Botanic Artisan offers paediatric naturopathic care in Surry Hills and via telehealth across Australia.
Disclaimer
The information provided in this blog is for your personal or other non-commercial, educational purposes. It should not be considered as medical or professional advice. We recommend you consult with a GP or other healthcare professional before taking or omitting to take any action based on this blog. While the author uses best endeavours to provide accurate and true content, the author makes no guarantees or promises and assumes no liability regarding the accuracy, reliability or completeness of the information presented. The information, opinions, and recommendations presented in this blog are for general information only and any reliance on the information provided in this blog is done at your own risk. Any third-party materials or content of any third-party site referenced in this blog/article/handout do not necessarily reflect the author’s opinion, standards or policies and the author does not assume any liability for them whatsoever.